
18 Comments
Several years ago, my colleagues and I analyzed the diversity of disease research supported by NIH’s National Heart, Lung, and Blood Institute, and wrote about the importance of maintaining a diverse scientific portfolio. In times of scarce resources, it is tempting to prioritize investments that seem to offer a better promise of direct returns. In my current position as NIH’s deputy director for extramural research, I still feel strongly that maintaining a strong commitment to long-term goals and maintaining a diverse science portfolio ultimately balances risk and long- versus short-time pay-offs.
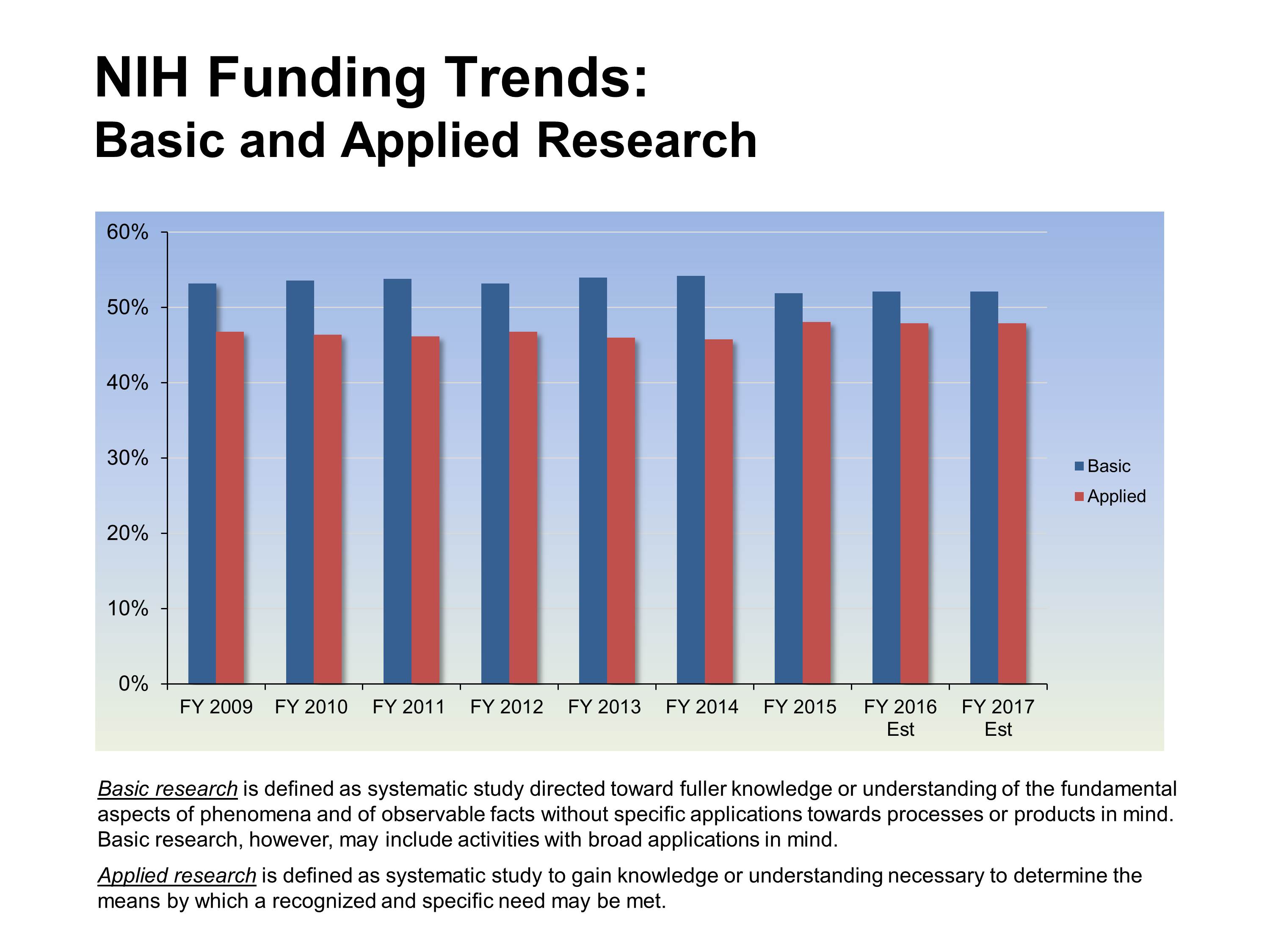
Basic science is an essential component of this diverse portfolio. NIH’s mission is to seek fundamental knowledge about the nature and behavior of living systems and the application of that knowledge to enhance health, lengthen life, and reduce illness and disability. This fundamental knowledge is obtained through research that addresses a specific health need, as well as through basic research that supports a broad understanding of human behavior and biology. Over half of NIH’s research funding supports basic research, as shown in the figure below provided by the NIH Office of Budget. We have heard that some think that NIH’s interest in supporting basic science is waning; indeed, there are some indications that this belief is driving a decrease in the number of basic research applications submitted to NIH.
All of the NIH institute and center directors, along with myself and other NIH leaders, joined NIH Director Francis Collins in signing a letter to the editor of Science, reiterating NIH’s commitment to basic science. We have also clarified application instructions for the public health relevance statement, to better reflect NIH’s mission and NIH’s support of a diverse research portfolio that may have short-term or long-term contributions to human health. Specifically, the instructions now read,
Using no more than two or three sentences, describe the relevance of this research to public health. For example, NIH applicants can describe how, in the short or long term, the research would contribute to fundamental knowledge about the nature and behavior of living systems and/or the application of that knowledge to enhance health, lengthen life, and/or reduce illness and disability.
It is our hope that this clarifies addressing how your research supports NIH’s mission, and reaffirms our commitment to the full breadth of scientific research.
One of the more interesting points in the Science letter is the finding that basic research applications to NIH have declined. I suggest that NIH examine its own data to determine if the decline is predominantly due to decreasing basic science applications from private medical schools and other soft money institutions. Although the decrease in success rates has been difficult for everyone, it has been especially painful for faculty that must generate the majority of their salary from research grants. Because of the requirement to pay most of their own salaries, many of these faculty need two grants in order to hire personnel to actually perform the research. As the grant success rate has plummeted, I have watched several faculty first lose one grant, then enter a death spiral since the school forces them to fire the people needed to be competitive for renewing the remaining grant. The end result is a shuttered laboratory.
Again, NIH already has data that basic science applications have dropped. It should be easy to determine whether or not the decline is similar across all types of institutions. The answer could be very informative.
Absolutely agree with you! We are totally on soft money from grants, and cannot be promoted without them. I just got my first one, and I support myself and one PhD researcher on it, with the rest going for lab supplies, publication costs, meetings, equipment and maintenance of it, etc. I would love to have another person or a student, but right now I am just worried about getting renewed, or the two of us are out of a job…
We do not doubt the NIH’s conceptual commitment to “basic research”. However, every policy that the NIH uses to manage basic research projects, from the structure of procedures used by the Center for Scientific Review to the latest version of the NIH biosketch, prevents any such commitment from being realized. This can be contrasted with analogous procedures at the NSF, NASA, and other agencies that successfully identify and support basic research. Further, there appears to be no mechanism for the community to give the NIH feedback on these issues.
It might be helpful to note that the change in the instructions for the Narrative (Public Health Relevance Statement) applies to the new forms (Version D) and not to Version C which is still in use through May 24, 2016.
my last two grant were not funded mainly due to the fact that my researcg is basic science. the main comment in the discussion summary was that prresented research is a need model ststem that allows to investigate the cells of onterest basic immunology BUT IT IS Not a model of any human disease, which significantly decreases. euthudiasm for this proposal. that is it, my grant was killed, there is no revocery from that. second unrelated project, again badic sience, different NZiH Institute. some comment this is not a how human infection happens. alrhough neet model, iit will not enhance knowlidge of any. human infection. review your study sections comments, instruct reviewers, monitor this. you already are not supporting badic science
Perhaps it would be useful to inform study section reviewers of NIH’s commitment to fund basic science. Otherwise, it’s just lip service and directly insulting to those engaged in basic research.
There are two problems here.
One is that “basic science” is nowhere defined with the rigor that a disciplined historian and philosopher of science would display. Characterizing the molecular mechanisms of a developmental process may appear devoid of immediate translational utility but is not necessarily “basic”. It is often still descriptive and epistemologically similar to much of translational science. True basic science would seek to understand FUNDAMENTAL PRINCIPLE of life that are matheaztically irreducible – a domain of research hardly ever touched upon by NIH, not even at NIGMS.
Second, unfortunately despite well-meant and well-formulated program descriptions and instructions to reviewers, the majority of reviewers does not possess the intellectual capacity to comprehend and embrace the spirit of such abstract announcements and to implement them in their review process. If they themselves do not see any impact and do not understand the elementary questions asked by the applicant, they automatically blame the applicant, using the lack of clinical significance as excuse (Who has not seen this standard ‘WEAKNESS” criticism: “.. however, it is not clear how this will impact patients…”)
I would like to second SWS’s comments. It seems disingenous of the NIH Institute and Center directors to bewail the decline in applications from basic researchers when their own policies have the effect of diverting funds from small labs and towards applied studies involving collaborations between clinical, translation and public health scientists. The applied researchers can survive in hard times by shifting effort between many sources of support in which each investigator plays minor roles, while most basic scientists need two R01’s to support their own salary, a few postdocs or students, and supplies. The recent moves towards MIRAs (essentially two R01’s combined into one and then cut) and budget caps continue to undermine basic researchers. Moreover, applied research is often done by medical fellows, while basic research is done by graduate students. NIH policies are hardly encouraging to graduate students, which bodes ill for the longer term future.
The message that NIH is committed to basic science is reassuring. But, in several ways, that message is undermined in the grant review process. “Significance” has come to mean translation to a therapeutic for a human disease. I sat on an NIH study section where a reviewer criticized basic science grants by saying, “I don’t see how this helps at the bedside.” Another sign is the denigration of model organism research. Notwithstanding the magnificent pioneering work of people like Randy Schekman and Robert Horvitz, there is quite a lot of pressure from NIH peer reviewers to steer away from model organisms and work with human tissue or iPS cells.
Last year, NIH leadership announced that the NIH gave more money to medical schools for basic science research than it gave to basic science departments. I think it is time the NIH carefully evaluated it’s policy of shifting “basic science” research funding to medical schools in support of translational science. We need answers to several questions: 1. Has this led to higher quality science? 2. Has this indeed facilitated translation to the clinic, as intended? and 3. Is the academic business model associated with this funding paradigm cost effective? If the answers to these questions are affirmative, then we need to start re-thinking how we prepare our students who are interested in academic research careers. On the other hand, NIH leadership has pointed out that increasing the number of NIH grants held by a PI does not lead to an expected scaling of scientific productivity or quality. Since PI’s in medical schools can hardly survive on a single grant, is it possible that lower productivity correlates with medical school funding (which might not be surprising, since faculty in medical schools must arguably spend more of their time raising money)?
Following the lead of Jeremy Berg, Jon Lorsch seems to be doing an excellent job of trying to tie general funding decisions with outcome metrics. Since expanded funding for translational science research was initiated around 2002, sufficient time has elapsed for the NIH begin studying the impact of this funding philosophy on basic science research.
That NIH wishes to support basic science is reassuring, but the passive and dull approach to implementing this initiative accross all institutes of NIH alraedy signals that NIH is not serious about it.
Both as a basic science RO1 grant applicant and a reviewer on NIH study sections, I find that the comment by S.H. above is very true. True basic science applications seeking to understand FUNDAMENTAL PRINCIPLE of biological processes is not supported by majority of reviewers on review panels for wide-ranging excuses as detaild by other responders. Perhaps these reviewers do not embrace the potential impact of fundamental knowledge gained and themselves do not see any clinical benefits to be realized. Basic reserach findings should potentially stimulate and envigorate additional and translational reserach.
If NIH is serious, it would be important to take definitive steps:
1. To change the composition of study panels to include basic reserach expertise accross the board.
2. To direct study section Chair, SRA and Program Officers for ensuring strict commitment of NIH to fund basic science.
3. Significance and Innovation sections for basic science grants should not be limited to an immediate translation to human disease or how patient care would change.
Unfortunately, today both SRA and Program Officers have come to recruit/complywith more and more translation oriented reviewerson their panels, perhaps the main cause of demise of basic reserach applications at NIH. Whatever happened to study panels like “basic biochemistry” or “molecular pharmacology” and “biophysics” at NHLBI? Who killed these panels?
If you talkers at NIH are serious about increasing success of basic science research applications, ACT NOW, make bold changes.
SsK has raised an interesting point. The reorganization that was done some years removed many basic science study sections. I believe that the idea was that many basic science applications would now be reviewed in the disease- or system-focused study section that was most relevant. The end result was that the remaining few basic science study sections became insanely competitive. Also, many of us have had the experience of sending basic science applications to more disease-focused study sections, only to find that it was reviewed by a panel with little or no real understanding of basic mechanisms and/or appreciation of basic science. It should be obvious from this blog and the former “Rock Talk” that many of us have come to view these and other NIH initiatives as destructive to basic research.
Let’s not fool ourselves: NIH never supported basic science as a matter of policy, at least, not during the last two decades. To be sure, without NIH support the world-leading position of this country in basic research would be actually unthinkable. This, however, happened not because of explicit NIH interest in basic research, but because such research was disguised as applied biomedical research, and tucked into funded R01s. Indeed, when the question of “translational significance” or “impact” is even asked (and PI has to answer it), it assumes applied research already. Further, R01 is hardly a proper framework for support for basic science: rather, it calls for accumulation of statistics to prove at the p<0.05 level the pre-existing discoveries already contained in Preliminary Data, and to test them in different conditions, according to narrowly formulated SAs. Real basic science, however, when conceived, does not have ready questions (let alone answers!); the questions continuously pop-up in the course of research. The only mechanism maybe related to basic science was the "high-risk" R21, but it eventually morphed into a little brother of R01 despite all efforts to the contrary. For sure, NIH understands all this very well, but in the current atmosphere, assigning any significant funds according to a long-term vision without declaring immediate tangible (and equitably distributed over the diverse general population) public benefits is a non-starter.
Many here have already commented on the disconnect between the stated support for basic science and the realities, especially in the reorganized study sections, where there is absolutely no training about how to evaluate basic vs. more applied research, and members apply their own priorities. An anecdote in this regard: On a study section, after I had argued for an application, a member questioned the application’s disease relevance. I answered that the application was for basic research squarely within the stated goals of the Institute, quoting the relevant sentence from the Institute’s website. The chair then said that he did not agree with those goals–Yes, that may be what this Institute says on its website, but really we (the reviewers) must see the immediate disease-relevant impact. Many heads in the room nodded, and another basic science application went down.
Putting more inclusive language online needs to be followed by training for reviewers.
I have been on many study sections in three NIH institutes and seen the very things listed above on multiple occasions. It is only going to stop when EITHER we make sure basic and clinical reviewers on review panels are equal in number, forcing mutual respect, OR we have the sense to restore separate clinical study sections and basic science study sections and budget studies in each area equally.
A further point we should consider is allowing reviewers comments to be viewed by the applicant between submission of initial review online and panel discussion, and a 1 page rebuttal be allowed on line within 24 hours. Reason why? Widely split scores (1,3,7 – as happened to a colleague of mine recently – and the primary reviewer loudly praised the application and its relevance and listed absolutely zero weaknesses) can easily be by a totally unqualified reviewer not understanding what is even being proposed, no matter how well written. Indeed in this case and in several of my own prior experiences the comments made by the person scoring 7 while others score ‘exceptional’ were unbelievably ill informed to a point I question their suitability as a reviewer at all. However when we took this to the PO and SRO we were stonewalled – take it up with CSR (??). Discussion triggered by a wide spread of scores would have revealed that immediately and forced the reviewers to justify high or low scores openly. A Basic study section would have prevented this happening altogether.
The final point is all of this would be less of a problem if NIH would do what it promised at the time CSR was created and cut the review cycle to 4 months, not 8 as it is now. At least we could do a fast turn around and resubmit.
I absolutely agree with the comments that there is limited appreciation or even understanding of basic research by reviewers – in a way, because we want fast and sexy results, “translational” research is preferred even though current evidence suggests that fast majority of such phenomenal translational studies never make it to the clinic due to unreproducibility (or other reasons). I think NIH/CSR needs to collect reviews from applications in the past several years and determine in what fraction one of the weaknesses listed is “unclear applicability of research to patient care”, and how many of such applications are actually funded. Also, this fraction could be looked over time and then we can determined whether NIH commitment to basic science (via reviewers) is real (which I suspect in reality is not)
Just to re-iterate to the NIH leadership team: instead of making claims, show us the relevant data that basic science research is appreciated and show how is this varied by study sections (whether basic science applications are rejected less over time)
Not only that this is often accompanied by a wide score spread. Analyzse the number of basic science grant where the intial score by the reviewer claiming the basic study ‘has little relevance to the clinic’ was 5 or more for approach while other reviewers who were trained in basic science scored 1-3 – and the grant was triaged. This has clearly happened to a colleague of mine recently . It seems now it only takes one bad score to triage and prevent discussion. In my opinion all grants receiving a 1-3 score from even a single reviewer should be discussed if only to get this out in the open. If the result is still a split and so an unfavorable score then fine, but if one person sees merit enough for a 1-3 score it should be discussed.